
-
Venous insufficiency occurs when the veins of the legs have difficulty sending blood back to the heart. Instead of flowing upward, blood tends to pool in the legs, causing heaviness, swelling, and discomfort at the end of the day. Over time, this can progress to spider veins, varicose veins, and in advanced stages, skin discoloration or even ulcers.
Varicose veins are enlarged, twisted veins visible under the skin, often appearing as blue or purple cord‑like structures on the legs.
Spider veins are a milder form. They are smaller, red or blue, and look like a fine “spider web” just beneath the skin surface.
Vein Anatomy and Venous Insufficiency
Veins and arteries have different roles.
Arteries carry oxygen‑rich blood from the heart to the body.
Veins return oxygen‑poor blood back to the heart.
Medical illustrations often show arteries in red and veins in blue, reflecting the natural color difference between oxygenated and deoxygenated blood.
The legs contain two venous systems:
Superficial veins, close to the skin (including the great saphenous vein on the inner leg and the small saphenous vein behind the calf).
Deep veins, located within the muscles.
These systems are connected by perforator veins. Most of the blood returns to the heart through the deep veins, which is why diseased superficial veins (such as varicose veins) can be safely treated or removed without harming circulation.
A key feature of veins is the presence of one‑way valves.
When leg muscles contract, they squeeze the deep veins and the valves open, pushing blood upward.
When muscles relax, the valves close to prevent blood from flowing backward.
If these valves become weak or damaged, blood leaks downward and accumulates in the veins. This increases pressure, stretches the vein walls, and further worsens valve function. This cycle is called venous insufficiency, and it leads to spider veins or larger varicose veins.
-
Several factors can increase the likelihood of developing venous insufficiency, varicose veins, or spider veins. These factors do not guarantee that the disease will occur, but they raise the overall risk.
Main Risk Factors
Inactivity (prolonged sitting or standing) — When the leg muscles do not contract regularly, the “muscle pump” is inactive, venous pressure rises, and blood tends to pool in the legs.
Obesity — Excess body weight increases pressure on the leg veins and worsens venous congestion.
Aging — Venous insufficiency becomes more common between ages 30 and 70. With age, the vein walls lose elasticity, making them more prone to dilation.
Female gender — Women are 2–3 times more likely to develop varicose veins due to hormonal influences (especially progesterone) and the effects of pregnancy.
Pregnancy — Hormonal changes weaken vein walls, and the growing uterus compresses central veins, increasing pressure in the leg veins. Veins often return to normal within a year after childbirth, but multiple pregnancies can lead to permanent varicose veins.
Leg injury — Trauma can damage veins and their valves.
Smoking — Increases the risk of venous thrombosis, which can destroy venous valves.
Deep venous thrombosis (DVT) — When a clot blocks or damages the deep veins, blood is diverted to the superficial veins. The increased pressure causes them to dilate and form varicose veins.
Pelvic mass — Rarely, a benign or malignant pelvic tumor can compress central veins, obstructing venous outflow and raising pressure in the leg veins.
Family history — Genetics play a significant role; venous disease often runs in families.
Understanding Risk
Having one or more risk factors does not mean a person will necessarily develop venous insufficiency. Some individuals with multiple risk factors never develop the disease, while others develop it without any identifiable risk factor — highlighting the importance of genetic predisposition.
Knowing your risk factors helps guide lifestyle choices and encourages appropriate medical monitoring.
-
People with venous insufficiency do not always have visible varicose veins. In many cases, the first signs are leg heaviness, fatigue, or mild swelling at the end of the day, which usually improves after resting with the legs elevated.
Common Symptoms
Heaviness or tired legs, especially in the evening
Mild ankle swelling that improves overnight
Spider veins or varicose veins
Night cramps
Burning, aching, or throbbing sensations in the legs
Symptoms worsened by heat or sun exposure
Spider veins and varicose veins are manifestations of underlying venous insufficiency. While they are usually not dangerous, they can be uncomfortable and may occasionally lead to complications such as bleeding or superficial thrombophlebitis (clot and inflammation in a superficial vein).
Skin Changes and Advanced Symptoms
Long‑standing venous insufficiency can affect the skin:
Dark brown discoloration (due to iron deposits from chronic congestion)
Thickened or fragile skin
Venous ulcers, which are painful sores that are slow to heal
For many people, varicose veins are also a cosmetic concern.
Relationship with Deep Vein Thrombosis (DVT)
Varicose veins occur in the superficial venous system and are not usually associated with deep vein thrombosis. However, in cases of severe varicose veins, there is a small increased risk of developing DVT.
A painful, swollen leg may indicate a DVT and requires urgent medical evaluation.
-
Spider veins and varicose veins are usually visible on the skin, but the severity of the underlying venous insufficiency cannot be assessed by appearance alone. A Venous Ultrasound is essential to confirm the diagnosis and determine the extent of the problem.
It is important not to begin any treatment before your vascular surgeon has evaluated whether venous insufficiency is present and how severe it is. This ensures that the treatment plan is complete, safe, and tailored to your specific condition.
Clinical Evaluation
Inform your vascular surgeon if you experience any symptoms such as heaviness, swelling, cramps, or burning sensations. Based on your medical history, the surgeon will perform a thorough physical examination and request a Venous Ultrasound.
Venous Ultrasound (Duplex / Triplex)
Venous ultrasound is:
Simple
Fast
Non‑invasive
Highly accurate
It allows the surgeon to:
Map the veins of the leg
Identify malfunctioning valves
Detect reflux (backward flow of blood)
Evaluate the deep and superficial venous systems
Ultrasound is also used during treatment, such as:
Endovenous laser ablation
Radiofrequency ablation
Foam sclerotherapy
Additional Imaging
In rare cases, if there is suspicion of central venous obstruction (in the abdomen or pelvis), your doctor may recommend a CT scan or MRI for further evaluation.
-
Not all cases of venous insufficiency require invasive treatment. When symptoms are mild and the venous ultrasound shows no significant reflux, management may be conservative.
Early‑stage spider veins or small varicose veins may be mainly a cosmetic concern, and it is entirely reasonable to seek treatment for aesthetic reasons—especially when the procedures offered are low‑risk.
More advanced cases, particularly those associated with skin changes or ulcers, typically require active treatment.
General Treatment Principles
Varicose veins are often treated by eliminating the diseased (“bad”) veins, which redirects blood flow into the remaining healthy veins. This improves circulation and reduces symptoms.
Many techniques exist, and advertisements may claim “unique,” “permanent,” “painless,” or “absolutely safe” solutions. In reality, several well‑established methods are available, each with specific indications.
Your vascular surgeon will guide you toward the most appropriate option based on:
Your symptoms
Venous ultrasound findings
The severity of reflux
Your personal goals (medical or cosmetic)
Main Treatment Categories
Lifestyle measures and medical management (compression stockings, leg elevation, exercise, weight control)
Sclerotherapy (Injection of a solution or foam to close small veins or spider veins).
Endovenous laser ablation (ELVA) (Minimally invasive technique using laser energy to seal the vein).
Radiofrequency ablation (RFA) Similar to laser, but using heat generated by radiofrequency.
Surgical treatment (vein stripping / saphenectomy) Removal of the diseased vein through small incisions; used less frequently today but still appropriate in selected cases.
All these options have a place in modern practice. The choice depends on the type of vein, the severity of reflux, and the overall clinical picture.
Learn more on the treatment options
(from Cleveland Clinic)
-
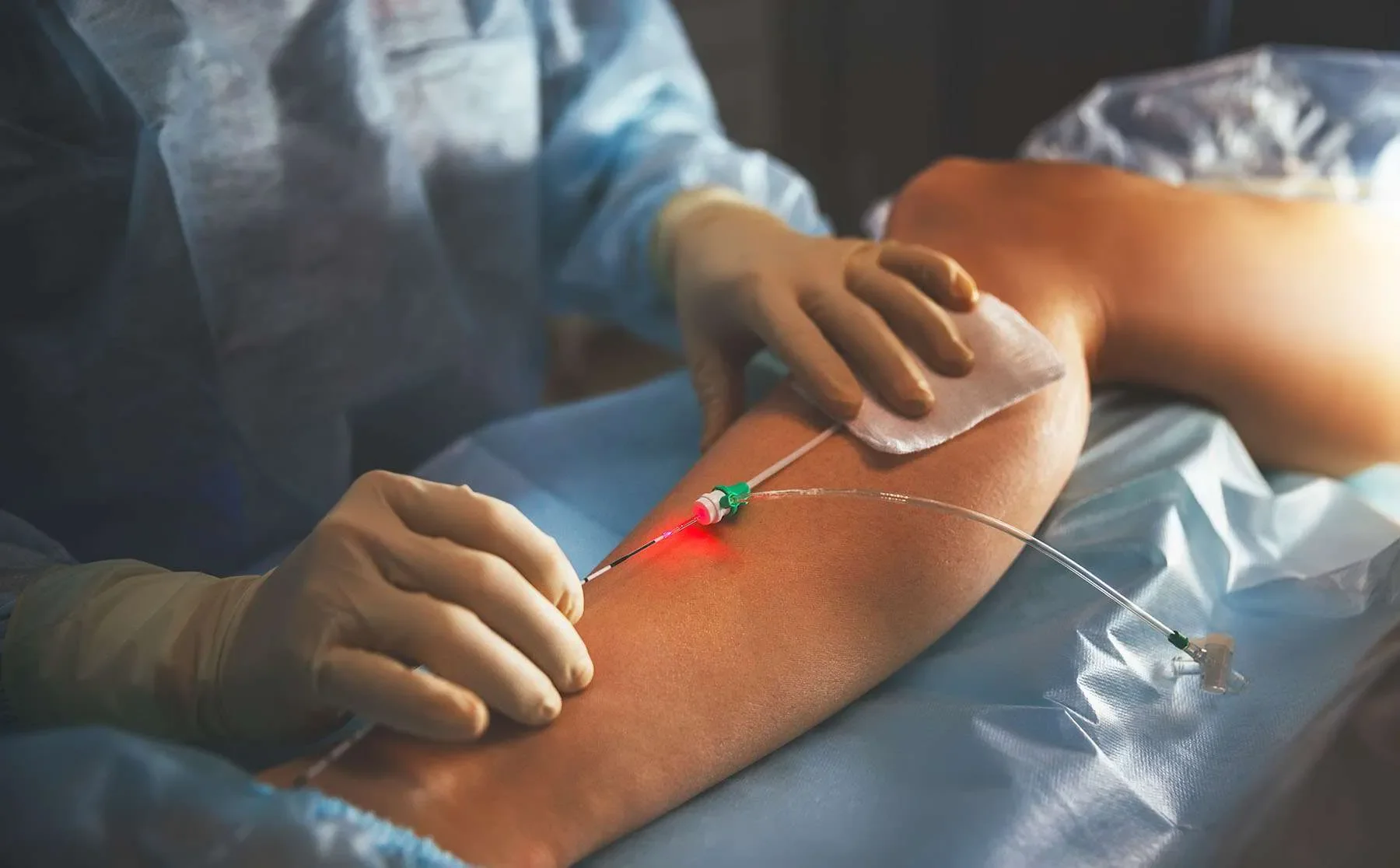
![Endovenous ablation (ELVA/RFA)]()
Endovenous ablation (ELVA/RFA)
Endovenous ablation (laser or radiofrequency) has replaced vein stripping for saphenous and other superficial venous insufficiency seen on ultrasound. Both methods are equally effective, have low complication rates, are incision‑free and can be done in the office, aiming at refluxing tributaries.
Under ultrasound, the diseased vein is punctured, a catheter placed, perivenous local anaesthetic injected, then laser or radiofrequency energy is applied to heat and close the vein.
A 2‑week follow‑up assesses need for adjunctive sclerotherapy or mini‑phlebectomy.
-
![Sclerotherapy (injections)]()
Sclerotherapy (injections)
Sclerotherapy is the most common treatment for spider and varicose veins, typically performed by angiologists or dermatologists and often following endovenous ablation or surgery to address remaining superficial veins. Before treating spider veins, clinicians must assess for underlying venous insufficiency and treat any incompetent feeder veins first.
The procedure uses a very fine needle to inject a chemical sclerosant that irritates the vein wall, causing it to collapse and be reabsorbed; for larger veins the sclerosant is often mixed into foam and injected under ultrasound guidance (foam sclerotherapy). Both liquid and foam sclerotherapy are essentially painless, with sessions typically lasting 20–40 minutes depending on the area treated.
A follow‑up at two weeks guides further sessions, as most patients require multiple treatments for optimal results.
-
![ambulatory mini-phlebectomy]()
Ambulatory mini-phlebectomy
Mini-phlebectomy (ambulatory, micro-phlebectomy or stab-avulsion): indicated for large varicose veins or when skin is unsuitable for sclerotherapy; often complements saphenectomy or endovenous ablation to remove residual veins and reduce sclerotherapy sessions.
Technique
Performed in clinic under local (or regional if combined) anesthesia.
Small 1–2 mm skin punctures; vein removed through micro-openings.
No sutures; scars minimal and usually invisible after healing.
Immediate discharge; return to activities the same day.
Advantages
Excellent cosmetic result
Immediate removal of prominent varicosities
Minimal pain, no stitches, tiny scars
Rapid recovery
Effective for bulky superficial varices not amenable to sclerotherapy alone
-
![]()
Surgical treatment (ligation / stripping)
Vein stripping (saphenectomy) is a traditional surgical treatment for varicose veins that remains useful for large, bulging varicosities when it may be more effective than endovenous techniques.
Performed under mild sedation, epidural or general anesthesia, the procedure passes a flexible wire through the diseased saphenous vein, ties and removes the vein through a small incision, with additional tiny incisions for tributary veins; the leg is then wrapped in compression. Most patients are observed for a few hours and go home the same day or next morning, can resume light activities immediately, expect mild pain and bruising for a few days, switch to a compression stocking after 2–3 days, and return for a two‑week follow‑up (sometimes with sclerotherapy for remaining spider veins).
-
![Conservative treatment]()
Conservative treatment
In many patients, symptoms of venous insufficiency improve significantly with simple, non‑invasive measures that relieve discomfort and slow disease progression. Conservative treatment is often the first step and continues to be valuable even when other interventions become necessary.




-
Several specialists may offer vein treatments, including dermatologists, angiologists, plastic surgeons, general surgeons, and vascular surgeons.
However, only vascular surgeons are trained in all treatment options and can therefore provide a complete and unbiased treatment plan.
Once a vascular surgeon has ruled out or treated any underlying venous insufficiency, procedures such as sclerotherapy or skin laser can be safely performed by other qualified practitioners (e.g., dermatologists, angiologists, plastic surgeons).
Always ask your doctor about their experience with the procedure you need. And remember:
“It’s not always about the procedure you want, but the procedure you need. It’s not always laser.”
-
While varicose veins cannot always be prevented, certain measures may reduce the risk or slow their progression:
Maintain a healthy weight
Exercise regularly
Elevate your legs when sitting
Avoid tight clothing around the waist, groin, or legs
Avoid high heels for prolonged periods
Avoid crossing your legs for long durations
These measures support healthy venous circulation.
-
Varicose veins may cause superficial vein thrombosis (superficial thrombophlebitis), which is usually benign.
Varicose veins are not generally associated with deep vein thrombosis (DVT) because they involve the superficial venous system.
However, in severe cases, there is a small increased risk of developing DVT.
A painful, swollen leg may indicate DVT and requires immediate medical attention.
-
After intense exercise, some people with varicose veins may feel more swelling, heaviness, or discomfort. The issue is the underlying venous insufficiency, not the exercise itself.
Exercise does not worsen varicose veins. In fact, it generally improves circulation. Activities such as walking or running activate the calf and thigh muscles, which act as a pump to push blood upward.
However, in advanced stages, symptoms may temporarily worsen during exercise (venous claudication).
Exercise is strongly encouraged for patients with varicose veins.
If symptoms worsen significantly, it may indicate progression of venous insufficiency or another cause that requires evaluation.
-
Wearing high heels daily for long hours is not recommended for women with varicose veins. High heels keep the calf muscles in a shortened position, reducing their pumping effect on the veins.
Wearing high heels occasionally, such as for social events, is not a problem.
Frequently Asked Questions
Still having questions ?
Book your appointment with Dr Psathas in Geneva and receive unbiased, expert vascular care
