
-
Peripheral Artery Disease (PAD) happens when the arteries in the legs become narrowed or blocked, most often because of atherosclerosis — the buildup of fatty deposits inside the vessel walls. These arteries start high in the pelvis, where the aorta divides into the iliac arteries, then continue through the groin as the femoral artery, behind the knee as the popliteal artery, and finally branch into the three small arteries that supply the foot. Together, they form the circulation that allows us to walk, stay active, and heal wounds.
When these arteries are healthy and open, the legs receive enough oxygen‑rich blood to meet the body’s needs, even during exercise. But as PAD progresses, one or more arteries can become so narrowed that blood flow is no longer sufficient. This can cause leg pain when walking, slow wound healing, and in very advanced stages, tissue loss or gangrene.
Atherosclerosis is the main cause of PAD. It is linked to smoking, high blood pressure, high cholesterol, diabetes, and age over 60, although genetics also play a role. Some people develop PAD without obvious risk factors, while others with several risk factors never do. Because the same process affects arteries throughout the body, PAD often occurs together with heart disease or carotid artery disease. Less common, non‑atherosclerotic causes include conditions such as Buerger’s disease and Raynaud’s phenomenon.
-
Peripheral Artery Disease (PAD) can develop silently for many years, especially in its early stages. Many people have no symptoms at all.
Some individuals may even have moderate or advanced PAD without noticing problems. This can happen when:
They have reduced pain sensation, as in diabetes with peripheral neuropathy.
The disease progresses slowly, allowing the body to form collateral circulation (natural bypass vessels).
They are not walking enough to trigger the increased blood flow demand that would reveal symptoms.
Intermittent Claudication — the Typical First Symptom
The most common early symptom is a tight, aching, squeezing pain or cramp in the calf, thigh, or buttock when walking a certain distance.
The pain disappears when you stop walking.
It returns at the same distance when you start walking again.
Over the years, this walking distance gradually becomes shorter.
This pattern is called intermittent claudication.
Other Possible Symptoms
Weak or tired legs
Difficulty walking or maintaining balance
Thin, shiny, or fragile skin on the legs or feet
Loss of hair on the feet
Wounds or sores that heal slowly
Thickened or opaque toenails (sometimes with fungal infection)
Erectile dysfunction in men
Advanced Stages — Critical Limb Ischemia
In severe PAD, pain may occur even at rest, especially in the foot or toes. This is called critical limb ischemia, meaning the limb is at risk due to severely reduced blood flow.
Critical limb ischemia is a surgical emergency. It may also present with:
Cold, numb feet or toes
Burning or aching pain when lying flat, relieved by sitting up
Pale color when the legs are elevated
Redness when the legs are hanging down (dependent rubor)
Reddish‑blue discoloration of the toes or foot
-
Peripheral Artery Disease (PAD) often progresses slowly and silently, especially in people who do not walk enough to trigger leg pain. For this reason, diagnosis relies on a combination of medical history, physical examination, and vascular tests.
If there are signs of critical limb ischemia, these tests are performed urgently. Always inform your doctor if you have experienced any of the symptoms described earlier.
Physical Examination
Your doctor will examine your legs and check the pulses at key points:
In the groin
Behind the knee
At the inner ankle
On the top of the foot
A weak or absent pulse suggests reduced blood flow and may indicate PAD.
Diagnostic Tests
• Doppler Ultrasound
A simple, non‑invasive test that evaluates blood flow in the leg arteries.
A handheld device sends ultrasound waves toward the moving blood cells. The returning signal produces a waveform and sound.
A faint or absent signal may indicate a blockage.
• Ankle‑Brachial Index (ABI)
A quick, non‑invasive, highly accurate test comparing blood pressure in the ankle with blood pressure in the arm.
A low ABI confirms PAD and helps assess its severity. It is useful for screening and follow‑up.
• Pulse Volume Recording (PVR)
Often performed together with the ABI.
Blood pressure cuffs are placed at different levels of the leg to measure changes in blood volume.
The results appear as pulsatile waveforms. Loss of pulsatility suggests an arterial obstruction.
This test is simple, fast, non‑invasive, and reliable.
• Peripheral Arterial Duplex / Triplex Ultrasound
A detailed ultrasound that visualizes the arteries, identifies the location of blockages, and estimates the severity of narrowing.
Non‑invasive, fast, and widely used.
• Computed Tomography Angiography (CTA)
A highly accurate imaging test providing high‑resolution 3D images of the leg arteries.
Useful for planning interventions.
It requires radiation and iodinated contrast dye, which may affect kidney function.
Not routinely ordered unless treatment is being considered.
• Magnetic Resonance Angiography (MRA)
As accurate as CTA, but without radiation.
If contrast is used (gadolinium), it is generally safer for the kidneys.
Limitations include higher cost, longer exam time, and contraindications in patients with claustrophobia or metal implants.
• Traditional Angiography
An invasive test performed in a surgical or interventional setting.
A catheter is inserted through the groin to inject contrast directly into the arteries.
It uses radiation and contrast dye.
Today, it is not routinely used for diagnosis, but becomes part of treatment when angioplasty or stenting is planned.
-
The treatment of Peripheral Artery Disease (PAD) depends on your symptoms, the severity of the disease, and your overall health. Management may include:
Lifestyle changes and medical therapy
Minimally invasive endovascular procedures (balloon angioplasty and/or stenting)
Open surgical repair (endarterectomy or bypass)
All three approaches have a role in modern vascular care. Your vascular surgeon will guide you toward the option that best fits your situation.
Treatment is individualized. In general, claudication (pain when walking) is treated conservatively unless it becomes severely limiting. Minimally invasive techniques are preferred when feasible, while open surgery is reserved for cases where endovascular treatment is not possible or has failed. For some patients in good overall health, open surgery may offer a more durable solution.
A thorough discussion with your vascular surgeon—reviewing risks, benefits, alternatives, and your personal preferences—will help determine the best plan.
Lifestyle Changes and Medical Treatment
Lifestyle modification and appropriate medical therapy are the foundation of PAD treatment, whether or not a procedure is needed.
Your vascular surgeon will work with you to:
Control blood pressure and cholesterol with medication (antihypertensives, statins) and dietary changes
Optimize blood sugar levels if you have diabetes
Start antiplatelet therapy (such as low‑dose aspirin or clopidogrel)
Support smoking cessation, which is essential
Encourage regular physical activity, especially daily walking, which improves walking distance over time
PAD does not “go away,” but proper medical treatment and lifestyle changes can slow or stop disease progression and allow the body to develop collateral circulation.
Regular follow‑up with your vascular surgeon is crucial, as the disease may progress even without symptoms.
Open Surgery (Endarterectomy and Bypass)
Open surgical treatment includes:
Endarterectomy — removal of the atherosclerotic plaque from inside the artery
Bypass surgery — rerouting blood flow using your own vein or a synthetic graft
Under general anesthesia, a small incision is made—usually in the groin or along the inner knee—at the site of the blockage. The artery is opened, the plaque is removed, and the artery is repaired. If the blockage is extensive, a bypass is created to restore blood flow.
Patients typically stay in the hospital 2–5 days after surgery. Some postoperative leg discomfort is expected but usually manageable with standard pain medication.
As with any operation, there are risks such as bleeding or thrombosis (clot formation), which can worsen ischemia. These risks should be discussed thoroughly with your vascular surgeon.
Angioplasty and Stenting
Angioplasty and stenting are minimally invasive procedures performed without a leg incision, through a small puncture in the groin.
Using X‑ray guidance, thin wires and catheters are advanced through the arteries to the site of the blockage. A balloon is inflated to open the artery. If the result is not optimal, a stent (a small metal mesh tube) is placed to keep the artery open.
Patients are usually treated in an outpatient basis (without hospitalisation) however one or two days stay in the hospital might be required depending on your overall health and the complexity of the procedure.
As with any intervention, angioplasty and stenting carry risks such as bleeding or thrombosis, which can worsen ischemia. These should be discussed with your vascular surgeon.
Learn more on the treatment options
(from Cleveland Clinic)
-
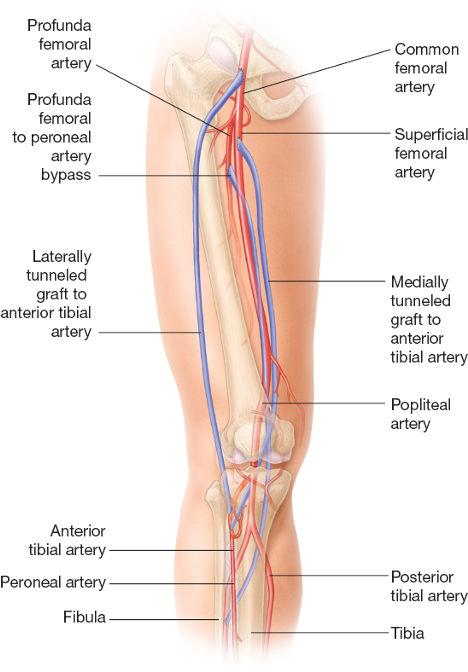
![Peripheral artery bypass]()
Peripheral artery bypass
A peripheral artery bypass is an operation to get your blood flowing again when a leg (or arm) artery has become narrow or blocked. This can happen when you have peripheral artery disease (PAD). Plaque made up of cholesterol and other fats can form an obstacle inside your artery. This makes it difficult for your blood to travel through it to deliver oxygen and nutrients to your tissues.
Your surgeon creates another route for your blood, allowing it to avoid the blockage. This is similar to building a highway that goes around a congested area. Your blood is like a car that can use the new highway instead of trying to get through a roadway jammed with cars.
-
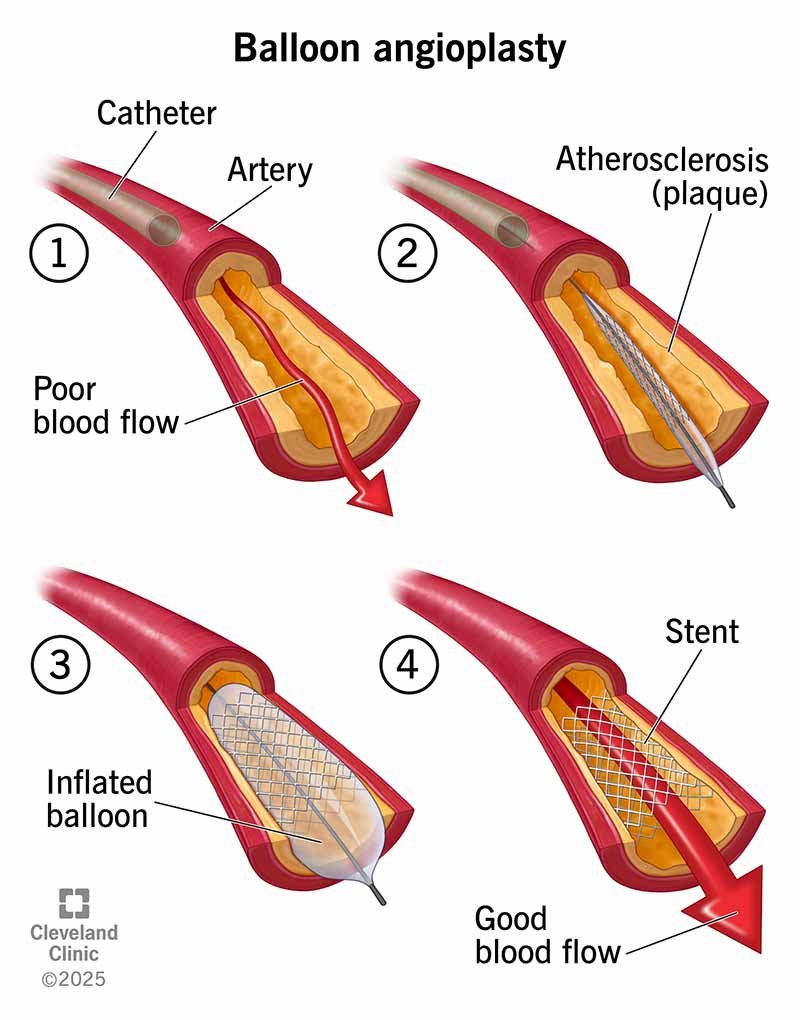
![Angioplasty and stenting]()
Angioplasty and stenting
Angioplasty is a minimally invasive procedure that opens arteries (large blood vessels) to let blood flow more easily. It most commonly treats atherosclerosis (a collection of plaque made of fat and cholesterol) in your arteries.
Angioplasty involves a tiny medical balloon that pushes plaque through in spots that are too narrow or blocked.
Angioplasties are generally safe procedures. They’re less invasive than other heart and vascular procedures, like bypass surgery.
Your cardiovascular health is very important to your overall health. Angioplasties are often necessary to try to prevent serious complications of atherosclerosis, like heart attack and stroke.
-
Peripheral Artery Disease can be treated by interventional radiologists, angiologists, and vascular surgeons.
Among these specialists, the vascular surgeon is trained in the full spectrum of vascular diseases and all treatment options—medical, endovascular, and open surgical. This allows for unbiased, comprehensive care tailored to your needs.
It is important to ask your doctor about their experience with the specific procedure being considered. And remember:
“It’s not always about the procedure you want, but the procedure you need.”
-
No. An abnormal screening result does not automatically mean surgery is required.
A physical exam may reveal absent pulses, and an arterial ultrasound (Duplex/Triplex) may show atherosclerotic plaques.
If these findings are mild or moderate, and you have no symptoms (such as leg pain or non‑healing wounds), surgery is usually not necessary.
Your vascular surgeon will recommend:
Appropriate medical therapy
Lifestyle changes
Yearly follow‑up to monitor progression
-
Regular exercise is one of the most effective treatments for PAD.
Patients with claudication (leg pain when walking) can significantly increase their walking distance through structured exercise. Training helps muscles use oxygen more efficiently and promotes the development of collateral arteries.
For best results:
Exercise at least 3 times per week
Each session should last 30–45 minutes or more
Daily walking is strongly encouraged and improves walking capacity over time.
There is no strict upper limit on exercise intensity. You may perform any activity you tolerate, as long as you protect your feet to avoid injuries.
-
Reduced blood flow means that even small injuries can become serious. Wounds may heal slowly and can lead to infection—especially in people with diabetes.
To protect your feet and legs:
Treat cuts, scrapes, or wounds immediately
Wear comfortable, well‑fitting shoes; avoid shoes that rub
Avoid tight socks or stockings that leave marks, as they worsen circulation
Keep your feet clean and moisturized to prevent cracks
Place cotton or wool between toes to reduce friction and absorb moisture
Check your feet regularly, including between the toes
If you notice an open sore, keep it dry, cover it with a non‑stick dressing, and contact your doctor promptly
Frequently Asked Questions

Still having questions ?
Book your appointment with Dr Psathas in Geneva and receive unbiased, expert vascular care