
-
A thoracic aortic aneurysm (TAA) is a bulging or widening of the upper part of the aorta caused by a weakness in its wall. The aorta is the body’s main artery, about 2 cm wide, carrying blood from the heart through the chest (ascending aorta, aortic arch, descending aorta) and then into the abdomen before splitting to supply the legs. An aneurysm can appear in any of these areas. When it affects the chest portion, it may involve the ascending aorta, the arch, or the descending aorta. If the abdominal part is also affected, it is called a thoraco‑abdominal aneurysm. Thoracic aneurysms are less common than abdominal ones, and the ascending aorta is the most frequent location.
Thoracic aneurysms can stay small and stable, or they can grow. The larger they become, the higher the risk of rupture, which is why regular monitoring is important. Treatment depends on size and growth rate and may range from simple follow‑up to planned surgery. Several factors can contribute to a TAA, including atherosclerosis (linked to smoking, high blood pressure, high cholesterol, and ageing), hereditary factors, and congenital or genetic conditions such as Marfan or Ehlers‑Danlos syndrome, bicuspid aortic valve, or coarctation of the aorta. Infections and trauma can also play a role. TAAs are more common in men and in people over 60.
-
Most thoracic aortic aneurysms cause no symptoms and are often found by chance during an X‑ray, CT scan, or MRI done for another reason.
As an aneurysm grows, it may press on nearby organs and cause:
Chest, back, neck, or jaw pain
Cough or shortness of breath
Hoarseness
Difficulty swallowing
These symptoms can easily be confused with more common conditions such as reflux or heartburn. If you experience persistent or unexplained symptoms, your vascular surgeon can help clarify the cause.
A sudden, severe chest or back pain may indicate a rupture, which is a medical emergency.
Rarely, small clots from the aneurysm can travel to the foot or toes, causing a cold painful foot or a blue painful toe.
-
A thoracic aortic aneurysm is often found by chance, usually during an X‑ray, CT scan, or another imaging test done for a different reason. If your doctor suspects an aneurysm, you will first have a medical history and physical exam. To confirm the diagnosis and measure the aneurysm, imaging tests are needed. A CT angiography (CTA) is the most accurate test and gives detailed information about the size and exact location of the aneurysm and its relation to the heart and the arteries to the brain and arms. It uses radiation and an iodine‑based contrast dye, which may not be suitable for people with kidney problems. This detailed information is essential when planning surgery.
Other tests may also be used. A magnetic resonance angiography (MRA) provides similar information without radiation, and its contrast dye is usually gentler on the kidneys, but the exam takes longer and may not be possible for people with claustrophobia or metal implants. An echocardiogram uses sound waves to look at the heart and the ascending aorta and is often used to screen family members. In some cases, to better see the descending aorta, your doctor may recommend a transesophageal echocardiogram, which involves placing a probe in the esophagus under light sedation.
-
Treatment for a thoracic aortic aneurysm aims to prevent complications, especially rupture, which can be life‑threatening. The best approach depends on the aneurysm’s size, growth rate, location, shape, your symptoms, and your overall health. Small aneurysms (usually under 5 cm) have a low risk of rupture and are often managed with regular monitoring, usually every 6–12 months with a CT scan or ultrasound. Your doctor will also help control blood pressure and cholesterol with medication, may recommend low‑dose aspirin, and will strongly encourage stopping smoking and maintaining a healthy lifestyle. Although an aneurysm cannot shrink on its own, good medical care can slow or even stop its growth. Rarely, even a small aneurysm may need treatment if it grows quickly, causes symptoms, or has a shape that increases rupture risk.
Larger aneurysms (typically above 5.5–6 cm) or those that grow rapidly usually require surgical repair, ideally planned before an emergency occurs. Two main techniques exist. Open surgical repair involves a larger incision in the chest to replace the weakened part of the aorta with a durable graft; recovery takes several weeks, but the repair is long‑lasting. Endovascular repair (TEVAR) is a minimally invasive option for most patients: a stent‑graft is guided through the blood vessels from the groin and placed inside the aorta to reinforce it. Recovery is usually faster, though lifelong imaging follow‑up is needed. In an emergency rupture, either open or endovascular surgery is performed immediately as a life‑saving procedure. Your vascular surgeon will guide you toward the safest and most appropriate option.
Learn more on the treatment options
(educational material for patients provided by the Cleveland Clinic)
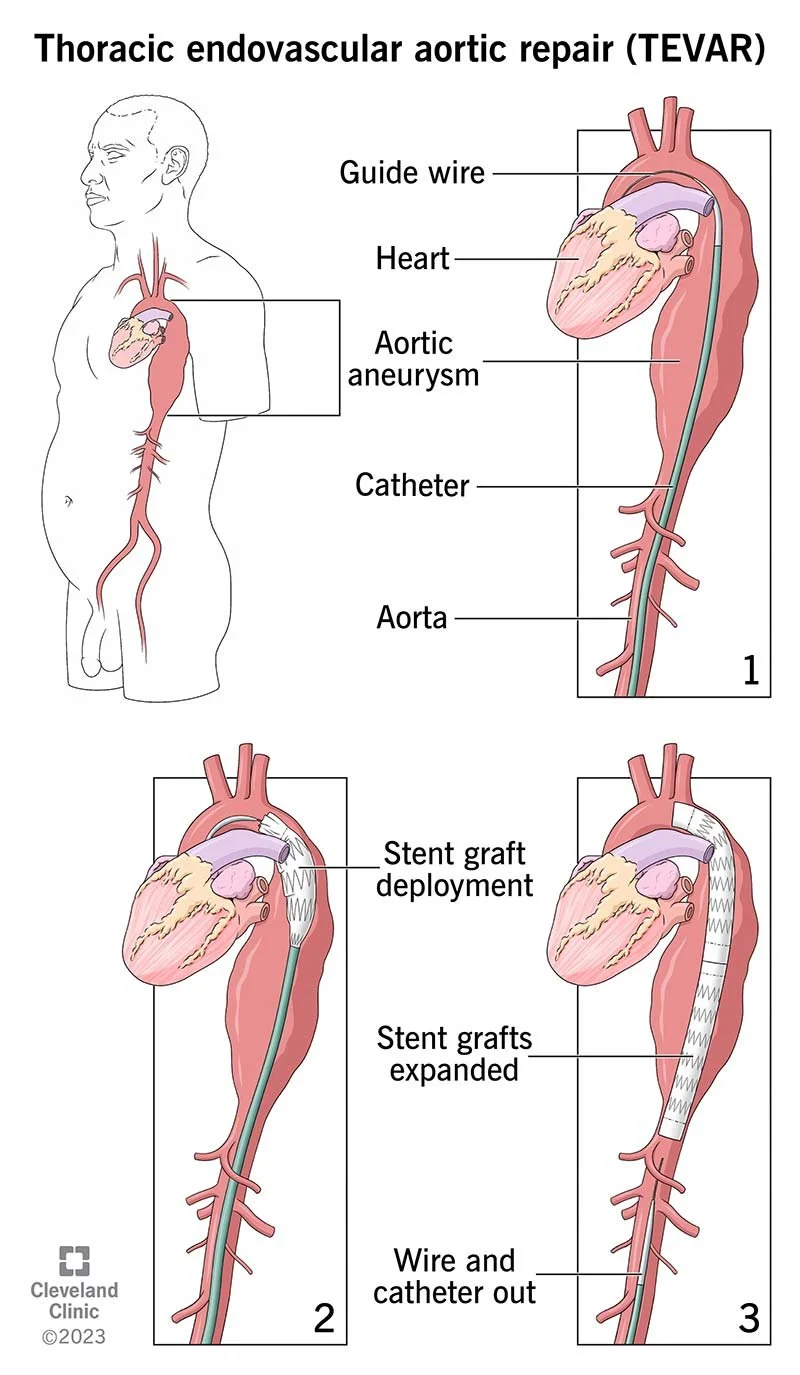
Thoracic endovascular aortic repair (TEVAR) is a minimally invasive procedure that treats descending thoracic aortic aneurysms.
An aneurysm is a weakened area of your artery wall that bulges outward and can lead to complications without treatment. TEVAR is generally safer than open surgery and offers a faster recovery in appropriate candidates.
In years past, surgeons used open surgery to treat thoracic aortic aneurysms and dissections. But they now prefer TEVAR in many cases. That’s because TEVAR has an easier recovery and a lower risk of serious complications in appropriate candidates.
Your surgeon will decide if you’re a candidate based on the anatomy of your blood vessels and other factors.
Frequently Asked Questions
-
Thoracic aortic aneurysms rarely give symptoms, till they grow big. Many are incidentally discovered as a result of medical imaging for other conditions, by echocardiogram, CT scans, MRI's, or even plain X-rays of the chest.
If you are over 65 or over 55 with a relevant family history you should discuss with your doctor and have an echocardiogram. It is safe, fast and painless.
-
Regular exercise is highly recommended with no major restrictions.
Avoid pushing, pulling or lifting anything more than 20-30 pounds. Also avoid contact sports
-
No. Endovascular repair is preferred option for the majority of patients, not though suitable for everybody. Open surgery versus endovascular repair relies upon the aneurysm anatomic characteristics.
Pushing the limits of endovascular repair, when unindicated, can result in multiple reinterventions and eventual need for open repair. Your vascular surgeon will guide you towards the best option.
-
Yes. Many people live for years with a stable aneurysm.
You may be advised to:
Keep blood pressure well controlled
Avoid heavy lifting or intense straining
Exercise moderately
Stop smoking
Maintain regular follow‑up scans
A healthy lifestyle helps slow aneurysm growth.
-
In most cases, yes. If your aneurysm is stable and monitored, flying is generally safe.
If you have a large or rapidly growing aneurysm, your doctor may recommend precautions or postponing travel.
-
Some aneurysms are linked to genetic conditions or run in families. If you have a strong family history, screening of close relatives may be recommended.
-
Call emergency services immediately if you experience:
Sudden, severe chest or back pain
Fainting
Difficulty breathing
Symptoms that feel “different” or alarming
These may indicate a tear or rupture.

Still having questions ?
Book your appointment with Dr Psathas in Geneva and receive unbiased, expert vascular care