
-
An abdominal aortic aneurysm (AAA) is a swelling of the main artery in your abdomen caused by a chronic weakening of the vessel wall. Most aneurysms grow slowly and cause no symptoms, but if they become large, they can burst and cause life‑threatening bleeding, a condition known as rupture. This is why early detection and monitoring are essential.
The main risk factors are smoking, high blood pressure, high cholesterol, age over 60, and family history. AAA is more common in men, but anyone can develop one. Some rare inherited conditions or infections can also weaken the aorta. A quick ultrasound scan can detect an aneurysm before it becomes dangerous.
-
Most people with an abdominal aortic aneurysm (AAA) have no symptoms at all. Many aneurysms are discovered by chance during an ultrasound, CT scan, or MRI done for another reason. Sometimes, a doctor may feel a pulsating mass in the abdomen during a routine exam. Because they often grow silently and can rupture without warning, AAAs are sometimes called “silent killers.”
When symptoms do appear, pain is the most common sign. It may be felt in the abdomen, back, chest, or groin and can be dull or severe. A sudden, intense pain in the back or abdomen may signal a rupture and is a medical emergency. Rarely, small blood clots from the aneurysm can travel to the foot or toes, causing a cold, painful, or blue toe. In unusual cases of infected or inflammatory aneurysms, symptoms like fever, weight loss, or problems with nearby organs may occur. Any of these signs should prompt urgent medical evaluation.
-
An abdominal aortic aneurysm (AAA) is often found by chance during an ultrasound, CT scan, or MRI done for another reason. Sometimes, a doctor may feel a pulsating mass in the abdomen during a routine exam. If an aneurysm is suspected, your doctor will review your medical history, examine you, and order imaging tests to confirm the diagnosis and measure its size.
The first test is usually an abdominal ultrasound — a quick, painless, and highly accurate way to detect or monitor an aneurysm. People over 55, especially smokers or those with a family history, are encouraged to have an ultrasound for early detection. For more detailed information, your vascular surgeon may request a CT angiography (CTA) or MR angiography (MRA). CTA provides the most precise images but uses radiation and contrast dye, while MRA avoids radiation but takes longer and may not be suitable for everyone. These detailed scans are essential for planning treatment when needed.
-
Treating an abdominal aortic aneurysm (AAA) is important to prevent rupture, which can be life‑threatening. The best treatment depends on the aneurysm’s size, growth rate, shape, location, and your overall health. Options include regular monitoring, minimally invasive endovascular repair (EVAR), or open surgical repair. Your vascular surgeon will help you choose the safest and most effective approach.
Small aneurysms (usually under 5 cm) rarely rupture, so they are monitored with ultrasound or CT scans every 6–12 months. During this period, controlling blood pressure, cholesterol, and stopping smoking are essential. Larger aneurysms (typically 5–5.5 cm or more) or those causing symptoms usually require surgery. EVAR uses small groin incisions to place a stent‑graft inside the aorta, allowing a faster recovery. Open repair replaces the weakened aorta with a durable graft through an abdominal incision and remains the best option for some patients. Both procedures carry risks, and EVAR requires lifelong follow‑up, so decisions are always personalized.
Learn more on the treatment options
(from Cleveland Clinic)
-
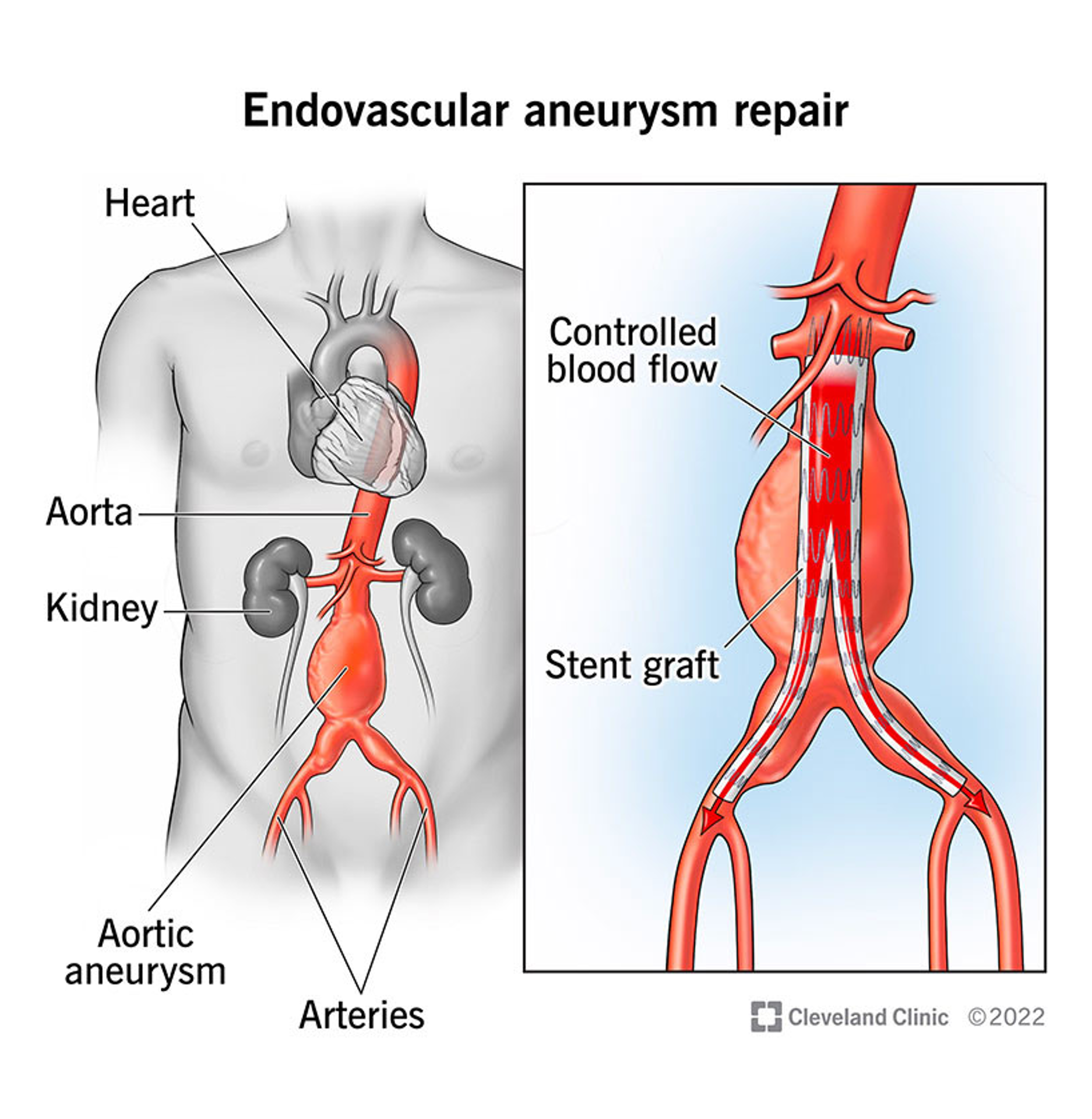
![Endovascular Abdominal Aortic Repair (EVAR)]()
Endovascular Abdominal Aortic Repair (EVAR)
Endovascular aneurysm repair (EVAR) is a minimally invasive procedure used to treat abdominal aortic aneurysms.
The aorta is the largest artery, carrying blood from the heart to other parts of the body. In the case of an abdominal aortic aneurysm, EVAR involves making small incisions and using specialised instruments to repair the bulge in the blood vessel.
The aim of EVAR is to prevent the aneurysm from rupturing, which can be life-threatening. The force of blood flow against a weak spot in the wall of the blood vessel causes the aortic walls to balloon outwards, creating an aneurysm. This can lead to rupture, disrupting blood flow to your organs. Life-threatening complications can occur within minutes.
EVAR reduces the risk of rupture by relining the aneurysm with a new tube, which takes the pressure off the aneurysm. This tube is called a stent graft and is made of fabric with a metal mesh frame.
-
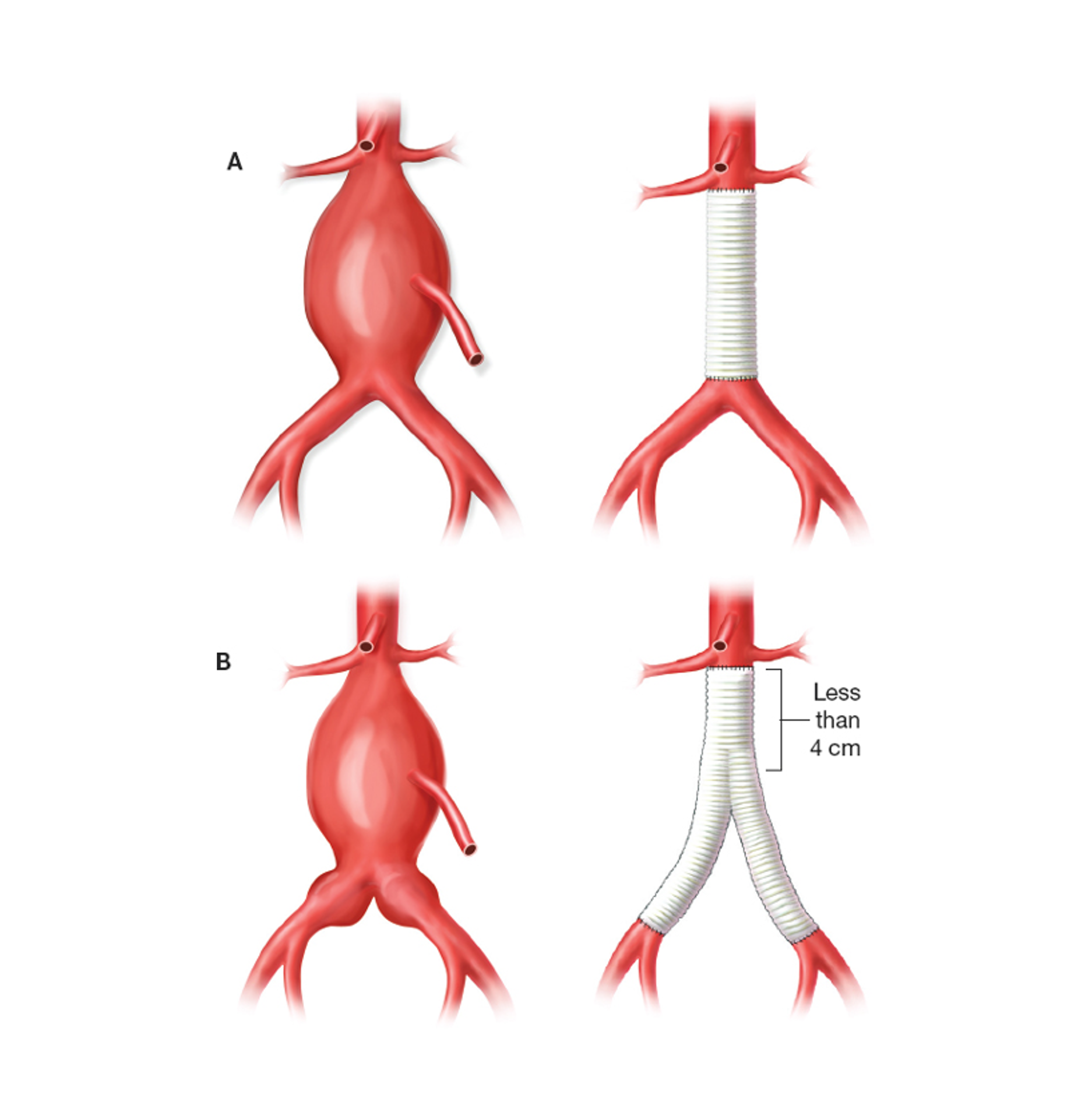
![Open Aortic Repair]()
Open Aortic Repair
Aneurysm surgery, also known as open surgery, is a treatment for aortic aneurysms. Aortic aneurysms damage your aorta and can cause life-threatening complications.
The main purpose of open surgery is to prevent rupture or dissection of the aneurysm. It can also repair damage resulting from such an event.
During the procedure, the vascular surgeon removes the damaged part of your aorta and replaces it with a synthetic fabric tube. This tube is called a graft. The graft functions as a new lining for your artery, allowing blood to pass through safely.
This procedure is performed by a vascular surgeon in a hospital operating theatre and is considered major surgery. To access the aneurysm, your surgeon needs to make a large incision in your chest or abdomen.
Aneurysm surgery is often necessary to prevent serious complications or death. As with any major surgery, it carries risks. However, the benefits usually outweigh the risks. Your vascular surgeon will discuss your options with you and establish whether you require surgery.
Frequently Asked Questions
-
Most aneurysms are found by chance during an ultrasound, CT scan, or MRI done for another reason. If you are thin and the aneurysm is large enough, you or your doctor may feel a strong pulse in your abdomen. Anyone over 65, or over 55 with a family history, should consider a simple, painless ultrasound screening.
-
No. Most AAAs grow slowly, only a few millimeters per year. When an aneurysm is under 5.5 cm, the risk of rupture is very low. Larger aneurysms carry a higher risk, and elective repair is usually recommended once the diameter exceeds 5–5.5 cm.
-
Regular exercise is encouraged. Avoid lifting more than 20–30 pounds and avoid contact sports. Otherwise, normal daily activities are safe for most patients.
-
Not always. EVAR is an excellent option for many patients, but suitability depends on the shape and anatomy of the aneurysm. In some cases, open surgery remains the safer or only option. Your vascular surgeon will guide you.
-
After open surgery, the diseased segment is replaced and cannot recur in the same spot. After EVAR, the aneurysm is excluded but not removed, so the stent‑graft can rarely move or leak. This is why lifelong follow‑up with ultrasound or CT is essential for all patients, especially after EVAR.
Still having questions ?
Book your appointment with Dr Psathas in Geneva and receive unbiased, expert vascular care
