
-
Carotid artery disease happens when the arteries in your neck become narrowed by fatty deposits. These arteries bring blood and oxygen to your brain, so when they get too tight — or when a small piece of plaque breaks off — the brain may not get enough blood. This can cause a mini‑stroke (TIA), which is temporary, or a stroke, which can lead to lasting damage of the brain.
Smoking, high blood pressure, high cholesterol, diabetes, excess weight and age over 60 all increase the risk, but family history also matters. Some people develop the disease even without clear risk factors. Because the same process affects arteries throughout the body, carotid disease often goes hand‑in‑hand with heart disease or poor circulation in the legs.
-
Carotid artery disease often develops quietly for years without any symptoms. The first sign may be a mini‑stroke (TIA), where symptoms last only minutes or hours, or a stroke, where symptoms can be permanent. Both can look the same at the beginning. Symptoms depend on the part of the brain affected and may include sudden vision loss, trouble speaking, weakness or numbness on one side of the body, loss of balance, confusion, dizziness or severe headache.
Any sudden appearance of these symptoms is a medical emergency. A TIA is a warning that a stroke may follow, and a stroke requires immediate treatment to protect the brain and improve the chances of recovery. The sooner blood flow is restored, the better the outcome.
-
Carotid artery disease usually causes no symptoms until a mini‑stroke (TIA) or a stroke occurs. To check for the disease, your doctor will review your medical history, examine you, and order imaging tests of the carotid arteries. Sometimes a doctor may hear a “bruit” — a whooshing sound in the neck — which can suggest narrowing, but this is not always present. If you have had symptoms such as sudden vision changes, speech difficulties or weakness on one side, it is important to mention them, as this guides the choice of tests.
Diagnosis is made with imaging. A carotid ultrasound is quick, painless and very accurate, and is often used for screening or follow‑up. A CT angiography (CTA) provides detailed 3D images but uses radiation and contrast dye, so it is mainly used after a confirmed event or before surgery. A MR angiography (MRA) offers similar accuracy without radiation and can detect small strokes, but it takes longer and may not be suitable for people with claustrophobia or certain implants.
-
Treating carotid artery disease is essential to lower the risk of stroke. The best option depends on your symptoms, how tight the artery is, the appearance of the plaque, and your overall health. Treatment may involve lifestyle changes with medication, carotid endarterectomy (open surgery to remove the plaque), or carotid stenting (a minimally invasive procedure using a stent placed through the groin). Narrowing below 50% is usually treated with medication alone, while significant narrowing — especially if symptoms such as TIA or stroke have occurred — often requires an intervention. Your vascular surgeon will help you choose the safest and most effective option for your situation.
Regardless of whether a procedure is needed, medical therapy and healthy habits are the foundation of treatment. This includes controlling blood pressure and cholesterol, taking aspirin or similar medication, stopping smoking, eating a balanced diet and staying active. Carotid disease does not disappear on its own, but proper treatment can slow or stop its progression and reduce stroke risk. Both endarterectomy and stenting usually require only a short hospital stay, and you will want to thoroughly discuss the benefits and risks of each approach with your vascular surgeon.
Learn more on the treatment options
(from Cleveland Clinic)
-
![Carotid endarterectomy]()
Carotid endarterectomy
A carotid endarterectomy is a surgery to remove plaque (fat and cholesterol buildup) from inside your carotid artery.
Carotid endarterectomy is a common carotid artery disease treatment. This helps prevent a stroke, which is the fifth leading cause of death.
If you have a stroke, it’s important to get to an emergency room for treatment within three to six hours to get the care you need.
-
![Carotid artery stenting]()
Carotid artery stenting
Carotid artery stenting is a procedure to open a blocked carotid artery. A blockage can increase your stroke risk. But getting the right treatment lowers this risk and helps you get back to your routine.
Transfemoral carotid artery stenting is a minimally invasive procedure to place a stent (small mesh tube) into the narrowed artery section. The stent improves blood flow, lowering your risk of stroke from carotid artery disease. Because it’s minimally invasive, you can typically return to your usual activities within a few days.
-
![Conservative treatment carotid]()
Conservative treatment
Regardless of whether a procedure is needed, medical therapy and healthy habits are the foundation of treatment.
This includes controlling blood pressure and cholesterol, taking aspirin or similar medication, stopping smoking, eating a balanced diet and staying active.
Carotid disease does not disappear on its own, but proper treatment can slow or stop its progression and reduce stroke risk.


Frequently Asked Questions
-
Carotid artery disease can be treated by interventional radiologists, neurologists, neurosurgeons and vascular surgeons. Vascular surgeons are the only specialists trained in all vascular diseases and all treatment options, which means they can offer truly unbiased advice. Always ask your doctor about their experience with the procedure you may need — and remember: it’s not about the procedure you want, but the procedure you need.
-
Not necessarily. An abnormal sound in the neck (a “bruit”) or plaque seen on ultrasound does not automatically mean surgery. If the narrowing is mild or moderate and you have had no stroke or TIA, treatment usually involves medication, lifestyle changes and yearly follow‑up. Your vascular surgeon will guide you.
-
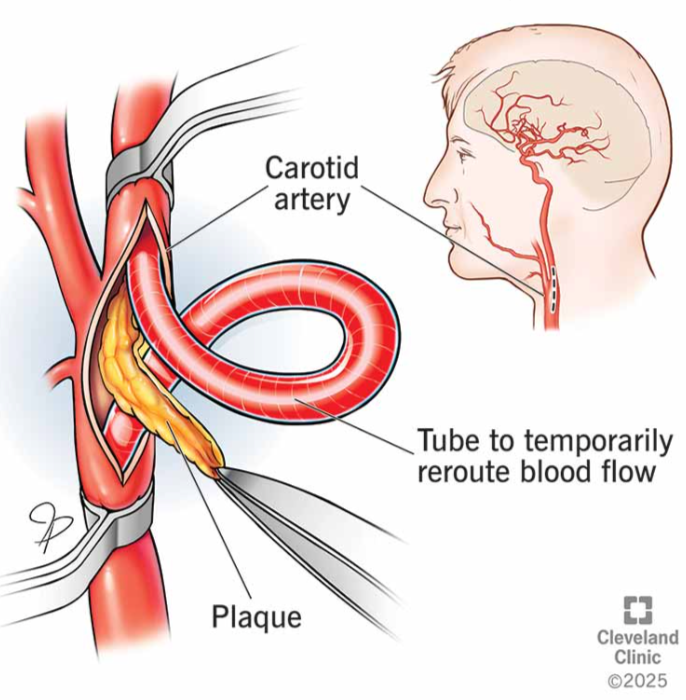
The brain has a natural backup system: several arteries work together to keep blood flowing even when one artery is temporarily clamped during surgery. Your surgeon monitors brain blood flow throughout the operation. If needed, a small temporary tube (shunt) is placed to keep blood moving while the plaque is removed.
-
Surgery greatly reduces the risk of stroke, but it cannot remove the risk completely. About one‑third of strokes are related to carotid disease; the rest come from other causes such as atrial fibrillation, small‑vessel disease or bleeding in the brain. This is why ongoing medical treatment and follow‑up remain essential.

Still having questions ?
Book your appointment with Dr Psathas in Geneva and receive unbiased, expert vascular care